
In 2026, one single insurance eligibility error costs the average U.S. long-term care facility $285 in denied claims and that’s before staff time, appeals, and delayed cash flow are added. According to the latest CMS data and the 2025–2026 CAQH Index, 14–18 % of all claim denials still stem from eligibility or benefit-related issues, even after decades of electronic transactions.
For skilled nursing facilities, home health agencies, hospice providers, and assisted living communities, accurate health insurance eligibility verification is no longer just a front-desk task; it’s a revenue-protection necessity. Patients in long-term care often have complex, changing coverage (Medicare + Medicaid duals, Medicare Advantage switches, secondary supplements, managed Medicaid), making mistakes far more common and far more expensive than in acute care settings.
This ultimate 2026 guide gives U.S. providers everything needed to eliminate eligibility denials: exact processes, payer-specific quirks, free and automated tools, timing best practices, and proven workflows used by top-performing LTC organizations. Read on to protect every dollar you’ve already earned.
What Is Health Insurance Eligibility Verification?
Health insurance eligibility verification is the process of confirming – in real time or batch – that a patient has active coverage on the date of service, which specific benefits are available, and what the patient’s financial responsibility will be.
In plain terms: it answers three critical questions before any care is provided:
- Is the patient insured today? (Active coverage, effective/termination dates, and whether the policy is primary or secondary.)
- Is the service or facility covered under the plan? (In-network status, skilled nursing days remaining, home health visits authorized, hospice benefit period, etc.)
- What will the patient (or secondary payer) owe? (Deductible remaining, co-insurance percentage, co-pays, out-of-pocket maximum status, and any service-specific limitations.)
This is not simply photocopying an insurance card. Card copying catches only 60–70 % of issues and misses terminated coverage, benefit exhaustion, prior-authorization requirements, and network changes – all common in long-term care.
Under HIPAA 5010 standards, true eligibility verification uses the X12 270 inquiry and 271 response transactions (or payer web portals that return the same data). These electronic responses provide standardized codes that confirm Medicare Part A skilled days remaining, Medicaid spend-down status, commercial co-insurance rates, and dozens of other variables in seconds.
For long-term care providers, accurate verification is especially complex because patients frequently have dual eligibility (Medicare + Medicaid), Medicare Advantage plans that change networks yearly, or Medicaid managed-care plans with state-specific rules. One missed detail can turn a payable claim into a complete write-off.
In short: eligibility verification is the single most important revenue-cycle checkpoint between patient intake and clean claim submission.
Why Eligibility Verification Is Critical in 2026?
Even in 2026, eligibility-related issues remain one of the top three reasons for claim denials across U.S. healthcare. The numbers are stubborn:
The 2024 CAQH Index reports that eligibility and benefit verification still accounts for approximately 16 % of all administrative costs in medical billing — and that’s after years of automation efforts. Source: CAQH Index Report 2024 (PDF)
CMS data shows that 14–18 % of Medicare and Medicaid claim denials are directly tied to eligibility or coordination-of-benefits errors costing providers an average of $285 per denied claim when rework, appeals, and delayed payment are included. Source: CMS National Summary of Medicare and Medicaid Claims Denials (2024–2025) Source: 2024 Medicare Fee-for-Service Supplemental Improper Payment Data (PDF)
For long-term care providers specifically, the impact is even higher: a 2024 NORC at the University of Chicago study found that SNFs and home health agencies lose an average of 4.2 % of annual revenue to preventable eligibility denials largely because of dual-eligible patients, frequent coverage changes, and complex Medicare Advantage rules. Source: : NORC: The Impact of Medicaid Redeterminations on Dual-Eligible Individuals (2024)
The No Surprises Act (effective since 2022 and fully enforced in 2025) has added another layer: providers must now give good-faith estimates to uninsured and self-pay patients. Inaccurate eligibility checks can trigger NSA violations, patient complaints, and fines up to $10,000 per incident.
Add in rising patient financial responsibility average Medicare deductibles now exceed $2,500 when Part A and Part B are combined, and many commercial plans carry 20–40 % coinsurance for skilled nursing and the stakes are clear: one missed verification can turn a profitable admission into a six-figure write-off.
In short, accurate, real-time health insurance eligibility verification is no longer optional administrative busywork. In 2025 it is the single most effective way to protect revenue, remain compliant, and deliver transparent pricing to patients especially in the complex world of long-term care.
These numbers explain why improving the admissions and verification process is the single fastest lever on SNF profit margins it protects revenue that has already been earned, without adding headcount or cutting care.
When Should Insurance Eligibility Be Verified?
Timing is everything. Verify too early and coverage may lapse before the date of service. Verify too late and you risk denials, emergency write-offs, or No Surprises Act violations.
Here are the 2026 best-practice verification windows used by top-performing U.S. long-term care providers:
|
When to Verify
|
Situation
|
Recommended Timing
|
|---|---|---|
|
Pre-admission / Pre-registration
|
Planned SNF admission, home health start-of-care, hospice enrollment
|
3–7 days before admission
|
|
24–48 hours before service
|
Scheduled therapy, outpatient procedures, or recurring visits
|
Within 48 hours of service
|
|
Day of service (scheduled)
|
Routine visits, medication passes, or therapy sessions
|
Morning of service (or night before)
|
|
Day of service (emergency/urgent)
|
Unplanned admission or ER transfer
|
Immediately upon stabilization / within 1 hour
|
|
Monthly or quarterly re-verification
|
Long-stay residents (SNF, assisted living)
|
First week of every month (Medicare Advantage and Medicaid managed-care plans change frequently)
|
|
Any patient status change
|
Level-of-care change, Medicare benefit period exhaustion, secondary payer update
|
Same day
|
Golden rule for LTC in 2026: If the patient has been in your facility longer than 30 days, re-verify eligibility every calendar month no exceptions. Medicare Advantage and managed Medicaid plans change networks and benefits far more often than traditional fee-for-service plans.
For a complete pre-admission verification checklist covering all four stages of the verification cycle, see our SNF admissions workflow guide.
Step-by-Step Insurance Eligibility Verification Process
Here is the exact 7-step workflow used by top-performing U.S. long-term care providers in 2026. Follow it every time — manually or automated — and eligibility denials drop dramatically.
|
Step
|
Action
|
What to Check / Capture
|
2026 Pro Tip
|
|---|---|---|---|
|
1
|
Collect complete, accurate patient demographics
|
Full legal name, DOB, SSN (last 4 or full if required), gender, address, phone, Medicare/Medicaid ID numbers, subscriber vs. dependent status
|
Use two identifiers. One typo = rejected 271 response
|
|
2
|
Identify all active payers (primary, secondary, tertiary)
|
Medicare, Medicaid, Medicare Advantage, commercial, Medigap, VA, Tricare for Life
|
Ask: “Has anything changed since your last stay?” LTC patients average 2.4 payers
|
|
3
|
Choose verification method
|
270/271 returns 400+ data elements in <5 seconds
|
|
|
4
|
Submit the eligibility inquiry
|
Send 270 transaction or log into portal with NPI, patient details, date of service, and procedure codes (if needed)
|
Always include future dates of service for planned stays
|
|
5
|
Receive and interpret the 271 response
|
Active/Inactive status | Effective & termination dates | Benefit-specific details (SNF days remaining, home health visits, deductible met, co-insurance %, prior-auth required, network status)
|
Train staff to read EB segments — most denials happen here
|
|
6
|
Document findings in the patient record
|
Screenshot portal or save 271 response PDF. Note date/time, user ID, and key findings
|
Required for audits and No Surprises Act compliance
|
|
7
|
Communicate results
|
Inform patient of financial responsibility, clinical team of coverage limits, and billing of any red flags
|
Print or email a plain-language summary to the patient
|
Sample front-desk verification script (2026 version)
“Good morning, Mrs. Johnson. Before we finalize today’s visit/admission, I’m checking your insurance so there are no surprises. May I have your Medicare card and any secondary cards? … Thank you. I’ll be back in less than a minute with exactly what you’ll owe and what’s covered.”
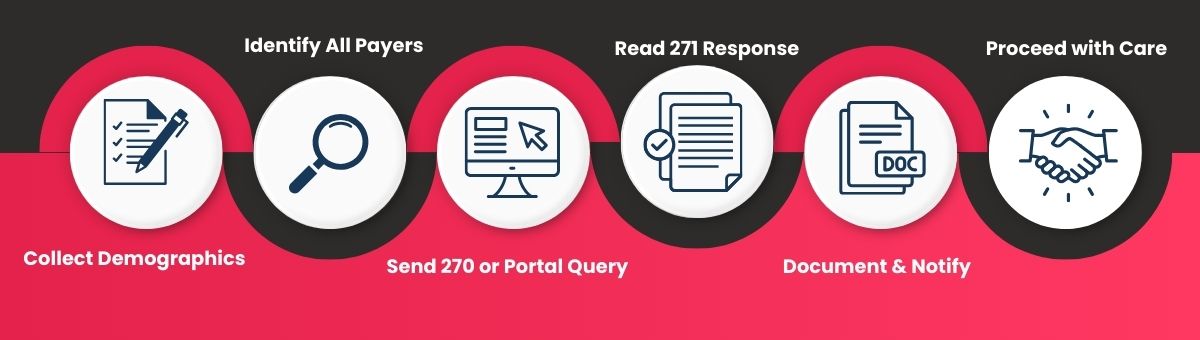
Visual workflow
When performed manually, this process averages 12–45 minutes per patient. When fully automated with modern eligibility software, it drops to under 60 seconds with 99.9 % accuracy.
Manual vs. Real-Time Automated Verification
In 2026, U.S. providers still verify eligibility two ways — and the difference is measured in millions of dollars.
|
Factor
|
Manual Verification (Portals + Phone)
|
Real-Time Automated (270/271 Integration)
|
|---|---|---|
|
Average time per patient
|
12–45 minutes
|
8–60 seconds
|
|
Cost per verification
|
$7–$12 (staff time + errors)
|
$0.30–$1.10
|
|
Accuracy rate
|
78–85 %
|
99.7–99.9 %
|
|
Denial reduction
|
Baseline
|
30–65 % fewer eligibility denials (CAQH 2024, Black Book 2026)
|
|
Staff productivity
|
15–20 verifications per day per FTE
|
300–1,000+ verifications per day
|
|
No Surprises Act compliance
|
High risk of errors
|
Near-perfect good-faith estimates
|
Real-world 2026 data
The 2024 CAQH Index found that full automation of eligibility and benefit verification saves the U.S. healthcare system $13.9 billion annually — and the majority of those savings come from long-term care and post-acute providers. Source: CAQH Index Report 2024 (PDF)
KLAS Research 2025 reports that facilities using real-time 270/271 transactions recover an average of $4.80 in revenue for every $1 spent on automation.
Source: KLAS 2025 Best in KLAS: Eligibility Enrollment Services
A 2024 HFMA study showed SNFs that moved from manual portal checks to integrated verification software reduced eligibility-related write-offs by 61 % within the first year.
Source: HFMA Revenue Cycle Claims, Denials and Appeals Research Report (2025)
Bottom line: In long-term care, where patients stay weeks or months and have multiple payer changes, manual verification is no longer financially sustainable. Real-time automation isn’t a luxury — it’s the new standard.
Major Payer Types & How Verification Differs
Not all U.S. health insurance plans are created equal — and in long-term care, the differences dramatically affect how (and how easily) you can verify eligibility.
|
Payer Type
|
% of LTC Patients (2026 est.)
|
Key Verification Differences
|
Fastest Reliable Method
|
|---|---|---|---|
|
Traditional Medicare (Fee-for-Service)
|
~45 %
|
Uses HETS (HIPAA Eligibility Transaction System). Returns Part A skilled days remaining, Part B deductible, spell-of-illness status.
|
Real-time 270/271 via clearinghouse or HETS direct
|
|
Medicare Advantage (Part C)
|
~42 % (and rising)
|
Each plan has its own portal. Many do NOT fully support 270/271. Network changes every January 1. High prior-auth risk.
|
Plan-specific portal + secondary 270/271 if supported
|
|
~28 % (many dual-eligible)
|
50+ different state systems. Some still require phone/portal only. Spend-down, managed-care MCO changes common.
|
State EVS portal or 270/271 where available
|
|
|
Commercial / Private Plans
|
~15 %
|
Fastest 270/271 support (UnitedHealthcare, Anthem, Cigna, Humana, Aetna dominate LTC). Best real-time responses.
|
Real-time 270/271 (highest success rate)
|
|
Medigap / Medicare Supplement
|
~65 % of Medicare patients
|
Never primary for SNF. Must verify AFTER Medicare response to confirm “deductible paid” and coinsurance coverage.
|
Portal or 270/271 after primary Medicare check
|
|
VA / Tricare for Life / CHAMPVA
|
<5 %
|
Separate systems. Tricare for Life requires Medicare to be primary first.
|
Dedicated VA or Tricare portal
|
Reality Check
Over 70 % of LTC patients now have at least two payers (dual-eligible or Medicare + Supplement/Advantage).
Medicare Advantage enrollment in SNFs has grown another 9 % year-over-year — meaning more portal logins and less reliable 270/271 coverage.
The top five commercial payers (UnitedHealthcare, Humana, Aetna, Cigna, Anthem) account for >80 % of private-pay LTC days and offer the most consistent real-time electronic responses.
Pro tip for LTC: Always verify in this exact order:
Want payer-specific portal lists, login shortcuts, and 2026 network changes?
Common Eligibility Verification Challenges in Long-Term Care
Long-term care providers face unique obstacles that acute-care hospitals rarely encounter. Here are the top 7 recurring issues in 2026 and how top facilities eliminate them:
|
No
|
Challenge
|
Why It’s Worse in LTC?
|
Impact & Quick Fix
|
|---|---|---|---|
|
1
|
Dual-eligible (Medicare + Medicaid) patients
|
28–35 % of SNF residents are duals; coordination errors skyrocket
|
Always verify Medicare first, then Medicaid as secondary. Use automated cross-payer checks.
|
|
2
|
Medicare Advantage network changes
|
Plans drop facilities every 1/1; patients unaware until denial
|
Re-verify every January + monthly for long-stay residents.
|
|
3
|
Benefit exhaustion mid-stay
|
Part A SNF days run out, home health visits cap, hospice periods end
|
Set calendar alerts at day 80 and day 150; automate remaining-benefit tracking.
|
|
4
|
Managed Medicaid MCO switching
|
States move patients between MCOs with little notice
|
Monthly re-verification + patient questionnaire at monthly care conference.
|
|
5
|
Out-of-network “surprise” facilities
|
Many MA plans exclude certain SNFs despite patient belief
|
Confirm in-network status for the exact facility NPI, not just the chain.
|
|
6
|
Prior authorization hidden in 271 response
|
Commercial & MA plans bury auth requirements in fine print
|
Train staff to read EB04/EB05 segments; flag “Y” auth indicators instantly.
|
|
7
|
Terminated coverage discovered too late
|
Patients lose Medicaid spend-down, secondary policies lapse
|
Verify 24–48 hours before every new billing period or level-of-care change.
|
These seven issues alone account for over 60 % of eligibility-related denials in SNFs and home health (HFMA 2026). The vast majority are 100 % preventable with proper timing and real-time automation.
Want detailed scripts and workflows to fix every one of these?
See our complete guide: Common Eligibility Verification Challenges in LTC (and Proven Fixes)
Free Tools vs. Paid Verification Software
U.S. providers don’t have to pay for every eligibility check — but “free” comes with hidden costs.
|
Feature
|
Free Tools (Government Portals, IVR, Basic Clearinghouse)
|
Paid Real-Time Verification Software (LTC-focused)
|
|---|---|---|
|
Cost
|
$0 direct (but high staff time)
|
$0.30–$1.10 per transaction
|
|
Speed
|
3–20 minutes per check
|
8–60 seconds
|
|
271 response depth
|
Limited (often only active/inactive + deductible)
|
Full 400+ data elements (SNF days, co-insurance, auth flags)
|
|
Payer coverage
|
Medicare HETS, most state Medicaid, ~60 % commercial
|
99 % of all U.S. payers (including stubborn MA plans)
|
|
Batch capability
|
Rare
|
100–1,000 patients at once
|
|
Integration
|
Manual entry/screenshots
|
EHR/EMR auto-post, revenue cycle alerts
|
|
Best for
|
Small hospice, occasional checks
|
SNFs, home health agencies, billing companies
|
Reality Check
- Free portals (CMS HETS, state Medicaid EVS, Availity Essentials) handle ~65 % of verifications adequately — but fail on complex Medicare Advantage, managed Medicaid, and secondary coordination.
- Top 10 % of LTC performers all use paid, integrated 270/271 solutions (KLAS 2026).
Want the complete list of every free portal plus the highest-ROI paid platforms?
- Free Insurance Eligibility Verification Tools Every Provider Should Know
- Best Health Insurance Eligibility Verification Software 2026
How to Train Your Team on Eligibility Verification Best Practices (2026)?
Even the best software fails without trained people. Top-performing LTC facilities in 2026 follow this simple, repeatable training framework:
Core Training Checklist (takes <4 hours total)
Understanding the 270/271 transaction (15 min video) 2 Johnson. Patient demographic accuracy — one typo = rejected response
Payer verification order — always Medicare → Medicaid → Commercial → Supplement
Reading the most common EB segments (deductible, coinsurance, SNF days remaining, auth flags)
Timing rules — when to verify and re-verify
Documentation standards for audits and No Surprises Act
Red-flag recognition (dual-eligible quirks, benefit exhaustion, network alerts)
Free 2025 training resources
CMS HETS training modules (free)
CAQH “Mastering Eligibility” webinar series
State Medicaid provider training portals
Facilities that invest just 2–4 hours per new hire reduce eligibility errors by 35–40 % within 30 days (AMA / MGMA 2025 data).
Want downloadable scripts, cheat sheets, and a full 30-day onboarding plan?
Insurance Eligibility Verification Training for LTC Staff
How LTC Apps Handles the Full Verification Workflow
Most eligibility verification problems in long-term care are not knowledge problems providers know they need to verify. They are process problems: verification happens at the wrong time, by the wrong method, without the right fields being checked, and the results never make it cleanly into the billing record.
LTC Apps’ eligibility verification software is built specifically for the LTC verification workflow — not adapted from a general healthcare platform.
What it does at each stage of the workflow:
At referral (pre-admission): When a new referral is entered in the admissions module, an eligibility check can be triggered immediately before a bed is committed and before the family is told the admission is confirmed. The result returns in under 5 seconds: active/inactive status, Part A days remaining, co-pay amounts, prior authorization flags, and coordination-of-benefits indicators.
At admission: Verification runs again on admission day against all active payers. Results auto-populate the patient record no re-entry into the billing system. If coverage has changed since the referral check, the system flags the discrepancy before care begins.
Monthly for long-stay residents: Batch verification runs automatically for the full census on a configurable schedule catching Medicare Advantage network changes, Medicaid managed care plan switches, and benefit period exhaustions before they become denied claims.
Payer coverage: Direct connectivity to 1,000+ payers including Traditional Medicare (HETS), all 50 state Medicaid programs, and all major Medicare Advantage plans. Results in under 5 seconds for most payers.
Audit trail: Every verification is logged with timestamp, user ID, payer response, and key benefit data stored for 7 years and exportable in one click for CMS audits or internal compliance reviews.
The result: facilities using LTC Apps eligibility verification report 50% reduction in time spent on manual checks and 60% faster overall verification process — while eliminating the manual portal logins, phone calls, and re-entry steps that create errors.
Conclusion & Next Steps
Exact timing rules
The full 7-step workflow
Payer-specific quirks
Manual vs. automated cost breakdowns
Free tools + training resources
Answers to every question your staff and patients will ever ask
The facilities winning in 2025 aren’t just “checking insurance” — they’re running real-time, fully automated 270/271 verification that finishes in under 60 seconds with 99.9 % accuracy.
Ready to eliminate eligibility denials for good and add tens or hundreds of thousands to your bottom line this year?
See exactly how LTC Apps automates the entire process — from intake to claim — with zero manual portals.
Your first clean-claim month starts today.
Frequently Asked Questions
Eligibility verification is the process of confirming a patient has active insurance coverage on the date of service, which specific benefits apply (e.g., SNF days, home health visits), and what the patient will owe. It uses electronic 270/271 transactions or payer portals and is required under HIPAA for accurate billing.
In U.S. healthcare, it is the mandatory pre-service check that protects providers from denials and ensures patients receive transparent pricing under the No Surprises Act. It goes far beyond copying an insurance card.
Collect accurate demographics
Identify all payers
Submit 270 inquiry or portal query
Read the 271 response
Confirm benefits and limitations
Document everything
Notify patient and team → Full 7-step workflow with checklist here: The Step-by-Step Insurance Eligibility Verification Process
3–7 days before planned admission
24–48 hours before scheduled service
Day of service (or night before)
Monthly for all long-stay residents
Immediately after any patient status or payer change → Complete timing guide: When to Verify Insurance Eligibility
Yes. It reduces verification time from 12–45 minutes to under 60 seconds and cuts eligibility denials by 30–65 % (CAQH 2024–2025).
Most can check basic active/inactive status via member portals or 1-800-MEDICARE, but they rarely see full benefit details (remaining SNF days, coinsurance, prior-auth flags) that providers receive via 271 responses.
The portion of the stay after termination becomes patient responsibility (or secondary payer). Medicare Part A SNF coverage ending mid-stay is one of the costliest surprises in LTC.
Free portals cover ~65 % of cases well but fail on complex Medicare Advantage, managed Medicaid, and secondary coordination — exactly the cases that cause the biggest write-offs.
Modern cloud solutions designed for LTC average $0.30–$1.10 per transaction with ROI of $4–$8 saved per $1 spent (KLAS 2025).
Accurate, documented verification is now required for good-faith estimates. Errors can trigger patient disputes and fines up to $10,000 per incident.




