Every month, the same conversation happens in skilled nursing facilities across the country.
The financial report lands in the administrator’s inbox. Medicare revenue is lower than projected. The Case Mix Index dropped from 1.71 last month to 1.59 this month. No explanation attached. No names. No context. Just a number that went the wrong direction.
Finance wants answers by end of day. The MDS coordinator says she’ll look into it. The DON isn’t sure where to start. And the administrator sits there knowing that whatever caused this didn’t happen this week. It happened 30 days ago, inside assessments that are already locked and submitted.
Your financial report is the last place you should discover a documentation problem.
Here is what that drop actually means in dollars. Using Illinois Medicaid rates as an example at a base nursing rate of $92.25, the difference between a nursing group weight of 0.85 and 0.52 is roughly $30 per resident per day. Across 15 Medicaid residents coded one group lower than their clinical picture supports, that is $450 per day. Over a 30-day month, that is $13,500 in legitimate revenue that documentation failed to capture. Not fraud. Not intentional error. Just a gap between what the clinical record showed and what the assessment locked in. The same math applies in every state the base rate changes, the problem does not.
That is what a CMI report does not show you. It shows you a number. It does not show you where the money went.
This article is about finding it.
If you need the foundation first how CMI is calculated, how PDPM weights work, what the HIPPS code chain looks like start with our Illinois SNF Medicaid CMI Reimbursement guide and come back here. This is the next conversation. The diagnostic one.
One more thing before we start. CMS flagged “case-mix creep” specifically in its FY2027 proposed rule, directing scrutiny at whether CMI movement reflects real resident acuity or documentation patterns. That changes the stakes. Getting your CMI right is no longer just a revenue question. It is an audit readiness question. Facilities that can show their documentation matches clinical reality are in a fundamentally different position than those that cannot.
Table of Contents
The Difference Between a CMI Report and a CMI Diagnosis
Every administrator gets a CMI report.
Almost none get a CMI diagnosis.
A report tells you the number changed. A diagnosis tells you which residents, which assessments, which specific documentation gaps, and which workflow broke down. Those are completely different conversations and most of the SNF industry is stuck having the first one.
The report goes to finance. The MDS coordinator does a general review. Some assessments get flagged as vague possibilities. Next month, the same thing happens again.
The facilities that hold their CMI consistently are not doing anything magical. They treat a CMI drop the way a physician treats an abnormal lab result. Not as a final answer. As the starting point for a specific investigation.
That shift from report to diagnosis is what this article is about.
The CMI Diagnostic Framework
Before we go into the specific reasons, it helps to understand the structure of the investigation.
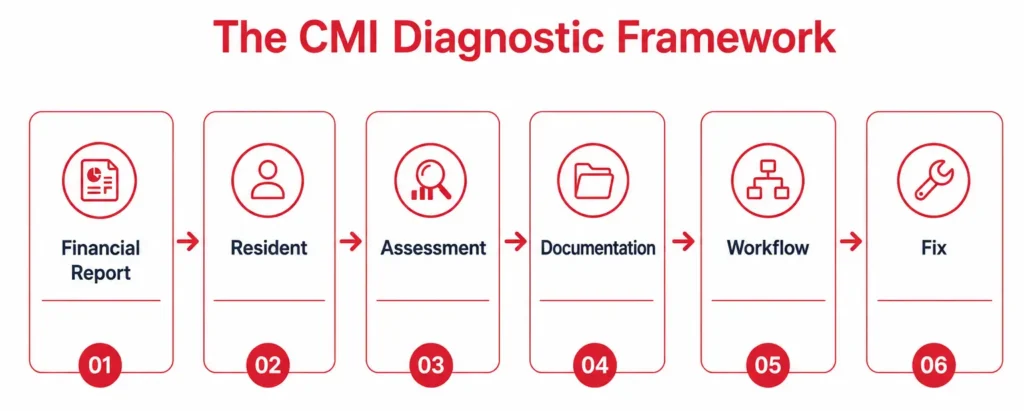
Every CMI drop traces back through the same chain.
Financial Report → Resident → Assessment → Documentation → Workflow → Fix
Most facilities stop at the first two steps. They see the report, they look at residents generally, and they make vague process promises. The facilities that actually fix the problem go all the way to the workflow level because that is where the drop was created, three to four weeks before the report arrived.
That is what the sections below are designed to do. Each reason follows the same structure so you can move from identification to correction as fast as possible.
Most facilities do not intentionally under-document acuity. The problem is almost always workflow timing, coordination, and incomplete clinical information at the exact moment the assessment is being finalized. Understanding that distinction matters because it tells you where to look for the fix.
5 Reasons Your CMI Dropped This Month
These are not the general explanations you will find everywhere else. What follows is the specific operational failure behind each cause the thing that actually happened inside your building.
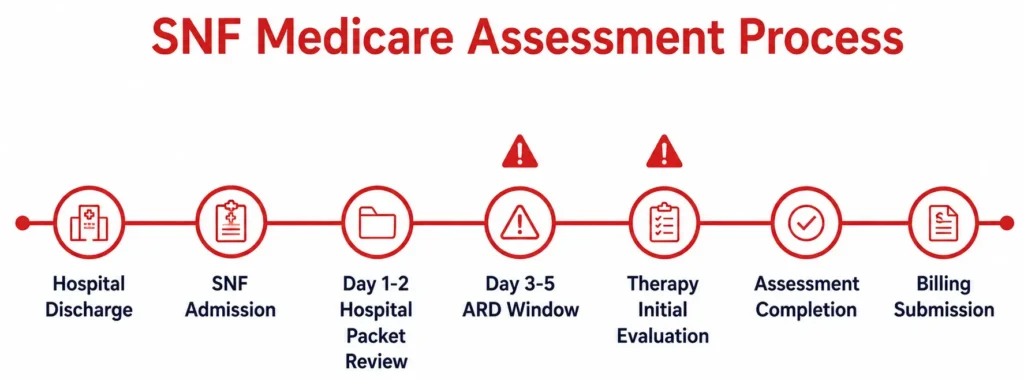
Reason 1: The ARD Was Set Before the Clinical Picture Was Complete
What happened
The Assessment Reference Date was locked on day 3 or day 4 because the MDS coordinator was managing a backlog and needed to stay on schedule. By day 3, therapy had not finished their evaluation. The hospital packet had not been fully reviewed. NTA comorbidities had not been documented from the transfer records.
The ARD closes the look-back window. Under the RAI Manual, the ARD defines the endpoint of the observation period for all MDS items. Everything that was not captured by that point does not exist for payment purposes even if it existed clinically.
What happened
The Assessment Reference Date was locked on day 3 or day 4 because the MDS coordinator was managing a backlog and needed to stay on schedule. By day 3, therapy had not finished their evaluation. The hospital packet had not been fully reviewed. NTA comorbidities had not been documented from the transfer records.
The ARD closes the look-back window. Under the RAI Manual, the ARD defines the endpoint of the observation period for all MDS items. Everything that was not captured by that point does not exist for payment purposes even if it existed clinically.
Why it hurts
The assessment reflects a resident who looks less complex than they actually are. Not because anyone coded it wrong. Because the window closed before the full clinical picture was in the record.
How to spot it
Pull the ARD date on your last 10 admissions. Compare it to the date of the therapy initial evaluation and the date the hospital records were received and reviewed. If the ARD precedes either of those dates, this is your problem.
How to prevent it
Build an ARD checklist into your admission workflow. The ARD should not be set until therapy has completed the initial evaluation and the hospital packet has been reviewed for NTA conditions. If the timeline is tight, use day 5. That one extra day is worth protecting.
Reason 2: Section GG Was Completed From a Single Observation
What happened
Section GG the functional scoring section that directly drives the nursing case-mix group is supposed to reflect what the resident can and cannot do across multiple observations during the look-back period. What I have seen happen, including at my own facility, is a nurse completing Section GG based on watching a resident attempt a task once during a busy shift. The resident was having a difficult morning. The nurse was rushed. The score came in lower than the resident’s actual functional baseline.
Why it hurts
Two or three points across multiple Section GG items does not sound significant. Across 15 Medicaid residents it can move your facility CMI more than most administrators realize. And it is not fraud. It is not malicious. It is inaccurate and inaccuracy costs money exactly the same way intentional errors do.
How to spot it
Compare Section GG scores from the assessment against nursing notes written during the same look-back period. If a nurse documented “resident ambulated 50 feet with supervision” but Section GG shows the resident requiring total assistance for ambulation, there is a discrepancy worth investigating.
How to prevent it
High-performing facilities treat Section GG accuracy as a revenue-quality metric, not simply a documentation requirement. Weekly MDS review meetings that cross-reference Section GG scores against nursing notes from the same period catch scoring inconsistencies before the assessment locks not after billing is already set.
Reason 3: The Admitting Diagnosis Code Was Not Specific Enough
What happened
Item I0020B on the MDS the primary diagnosis field is one of the most consequential single fields in the entire assessment. The ICD-10 code entered there maps to a PDPM clinical category that directly influences the nursing component classification. When that code is vague debility, muscle weakness, fracture unspecified the grouper has less to work with.
The hospital discharge summary almost always contains what is needed for a more specific code. Orthopedic fracture with complication. Sepsis resolving. Post-surgical wound requiring skilled nursing intervention. But if the MDS coordinator selects a generic code from a dropdown without cross-referencing the hospital record, the opportunity is gone once the assessment locks.
Why it hurts
A less specific ICD-10 code can place a resident in a lower clinical category under PDPM. That affects the overall HIPPS code and nursing classification. One vague code on one high-acuity resident can mean hundreds of dollars per day in uncaptured reimbursement.
How to spot it
Pull I0020B from your last 20 Medicare assessments. Open the hospital discharge summary for each one. Ask one question: is the code in the MDS the most specific code the discharge summary supports? If the hospital documented a specific condition and the MDS shows an unspecified variant, that gap has a payment consequence.
How to prevent it
Cross-referencing the hospital record against the MDS diagnosis code should be a standard step before any assessment locks. This is exactly what LTC Apps Medical Code Analysis was built to do surface the more specific diagnosis from the clinical record before the assessment closes, not after billing is already set.
Reason 4: Therapy Documentation Finished After the Assessment Window Closed
What happened
Therapy notes were running 24 to 48 hours behind actual sessions which happens at virtually every facility during high-census periods. The MDS coordinator finalized the assessment before the therapy record was complete. The clinical picture in the assessment does not reflect what therapy actually observed and documented.
Why it hurts
Therapy notes during the look-back period inform Section GG scoring and validate functional status. When they are missing from the record at the time of assessment completion, the MDS coordinator is working with incomplete information. The assessment reflects that incompleteness and the payment reflects the assessment.
How to spot it
Check the date of the last therapy note against the assessment completion date for your last 10 Medicare residents. If therapy notes were being entered after the assessment was finalized, this is a workflow sequencing problem.
How to prevent it
Therapy documentation deadlines need to be aligned with MDS timelines not treated as separate workflows. A simple rule that works: no assessment is finalized until the therapy notes from the look-back period are complete and in the record.
Reason 5: A Significant Change in Condition Was Not Recognized as an Assessment Trigger
What happened
A resident’s condition changed meaningfully mid-stay. A hospitalization and return. A new wound. A significant weight loss. An acute infection. The clinical team managed it. But nobody flagged it to the MDS coordinator as a significant change requiring a new assessment. The original assessment stayed active. The payment group reflected where the resident was three weeks ago, not where they are now.
Why it hurts
When a resident’s condition changes significantly and a new assessment is not triggered, the facility continues to be paid based on outdated clinical information. If the resident’s acuity increased — the most common scenario after a hospitalization — the facility is providing higher-acuity care at a lower-acuity payment rate.
How to spot it
Review your IDT meeting notes from the past 30 days. Was every hospitalization and return discussed as a potential significant change trigger? Was every weight loss of 5 percent or more flagged? If those conversations are not happening consistently, triggers are being missed.
How to prevent it
Build a significant change trigger checklist into your IDT meeting structure. Every clinical event that meets the RAI Manual criteria for a significant change should generate an automatic MDS review conversation — not an optional one.
Early Warning Signs Your CMI Was Already Falling
The CMI drop you saw in this month’s report was visible three to four weeks ago if you knew what to look for.
None of these signals require a financial report. All of them are visible in the daily workflow if someone is watching.
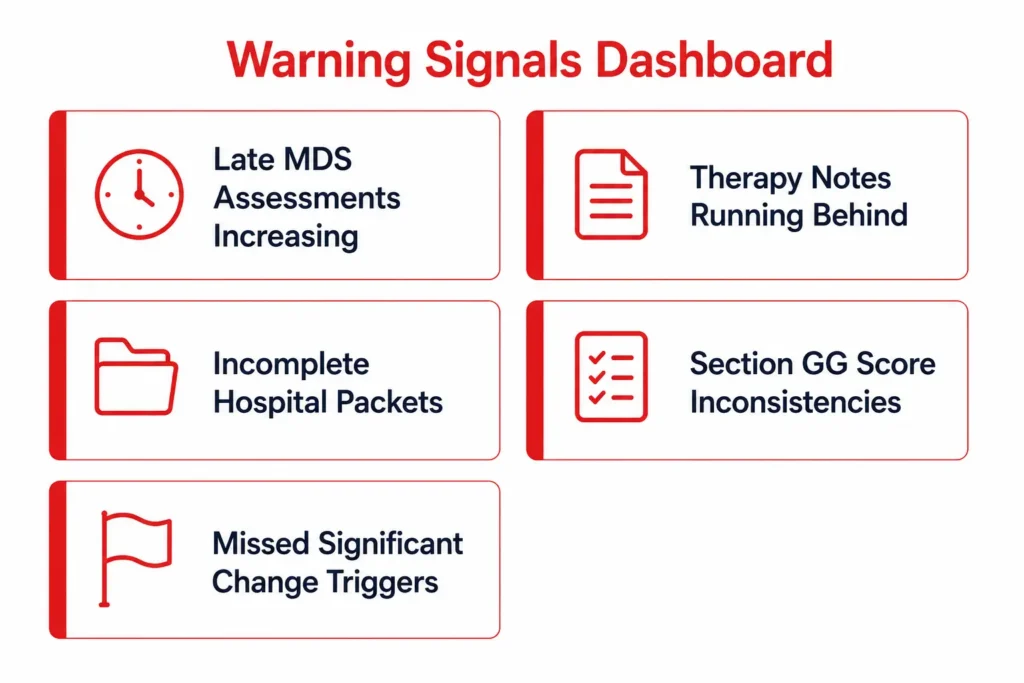
Your MDS coordinator’s open assessment count was climbing. More than two or three open assessments simultaneously creates backlog pressure. Backlog pressure drives early ARD decisions. Early ARD decisions cut off clinical information before it reaches the assessment.
Therapy notes were running consistently late. If your therapy team documents sessions the following day as standard practice, your MDS data is always working from an incomplete record. This compounds quietly over weeks before it shows up in a number.
New admission hospital packets were arriving incomplete. The transfer summary is the source document for NTA comorbidities and admitting diagnosis. If it arrives with missing pages and the assessment starts anyway, the revenue gap is built in before the resident has been in the building 48 hours.
Section GG scores were inconsistent across shifts. If day shift consistently scores residents differently than evening shift on the same ADL items, something is wrong with how the assessment is being conducted not with the residents.
Significant change triggers were not being discussed in morning meeting. A hospitalization return, a weight change, a new diagnosis these should generate an automatic MDS review conversation in the IDT. If that conversation is not happening consistently, triggers are being missed.
Every one of these signals is catchable before an assessment locks. After it locks, the revenue is set. The question is whether you catch the pattern this cycle or discover it when the financial report arrives.
How to Know Your CMI Will Drop Before Month-End
This is where the real opportunity is and where most facilities are not looking.
Most CMI management is reactive. The report arrives. The investigation starts. The process improvement happens. By the time it takes effect, two more monthly cycles have passed.
The facilities that hold CMI consistently track three leading indicators in real time before any assessment locks.
Open assessments by ARD proximity. Which assessments are within 48 hours of their ARD with incomplete Section GG or missing therapy documentation? That list, reviewed daily, tells you exactly where next month’s CMI risk is sitting right now.
Diagnosis code completeness on new admissions. Within 24 hours of admission, has I0020B been cross-referenced against the hospital discharge summary? If not, the coding gap is already forming.
Significant change trigger review by resident. Which residents had a clinical event this week that meets the RAI Manual criteria for a significant change assessment? Is the MDS coordinator aware of each one?
These three questions, answered daily, convert CMI management from a monthly investigation into a weekly workflow. The administrator who can answer them on a Tuesday morning will not be surprised by the financial report four weeks later.
How to Find Which Residents Are Pulling Your CMI Down
This is the part nobody writes about. Here is exactly how I do it.
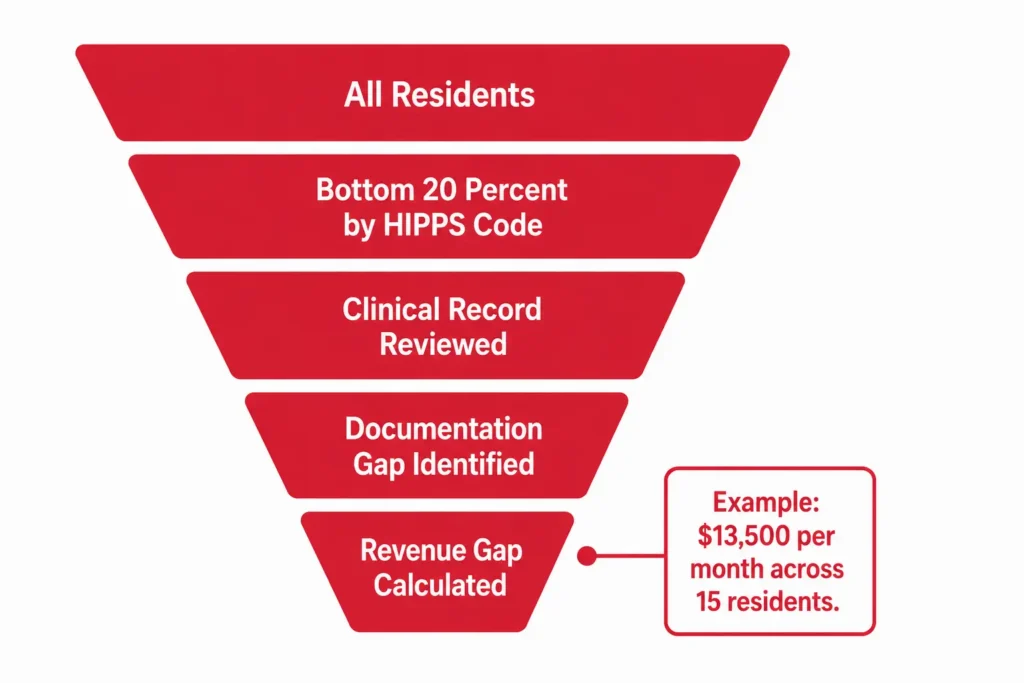
Step one. Pull your current MDS assessment data and sort residents by HIPPS code, lowest to highest. Your lowest HIPPS codes correspond to your lowest nursing case-mix weights. Those are your starting point not every resident, just the bottom 20 percent.
This is the part nobody writes about. Here is exactly how I do it.
Step one. Pull your current MDS assessment data and sort residents by HIPPS code, lowest to highest. Your lowest HIPPS codes correspond to your lowest nursing case-mix weights. Those are your starting point not every resident, just the bottom 20 percent.
Step two. For each resident in that bottom group, pull three things from their assessment: the I0020B diagnosis code, their Section GG functional scores, and their NTA comorbidity count.
Step three. Open the clinical record alongside the assessment not the MDS, the actual clinical record. Look at the hospital transfer summary, the nursing notes from the assessment look-back period, and the therapy evaluation. You are looking for one thing: does the clinical record show higher acuity than what the HIPPS code reflects?
Step four. Flag every resident where the answer is yes. This is your revenue gap list. Each flagged resident represents an assessment where documentation did not capture what was clinically present.
Step five. Calculate the weight differential for each flagged resident. Using Illinois rates as an example if a resident’s documentation placed them in a nursing group at a weight of 0.52 when their clinical picture supports a group at 0.85, that difference multiplied by the $92.25 base rate and the number of Medicaid days is the monthly cost of that single assessment gap. Do that across 10 residents and the number becomes a conversation you bring to finance except this time you are the one with the data.
Finding one resident takes 20 minutes. I can do that manually. Finding five is a morning’s work. Finding all at-risk residents across 130 beds before the current assessment window closes is a different problem entirely. That is not a time management problem. It is a scale problem. Manual processes do not solve scale problems they delay them until the financial report arrives.
What to Fix This Month
The assessments from last month are locked. That revenue is already determined. But the pattern that caused the drop is still active. Here is exactly what to do this week.
Hand this checklist to your MDS coordinator today.
Pull every assessment from the past 30 days where the HIPPS code landed in the bottom two nursing groups. Those are your starting candidates.
For each one, verify that Section GG scores are consistent with nursing notes written during the same look-back period. Document any discrepancies.
Check the ARD on each assessment. Was it set before or after therapy completed their initial evaluation? Note every instance where it was set before.
Review the I0020B diagnosis code against the hospital discharge summary for every new admission this month. Flag every case where the MDS code is less specific than the clinical record supports.
Identify every resident who had a notable clinical change this month hospitalization return, new wound, significant weight change, new behavioral symptoms. Did each one generate an MDS review conversation in your IDT? Document the ones that did not.
Review NTA comorbidities on your top 10 Medicare residents. Are all conditions documented in the hospital transfer summary also captured in the MDS?
Work through this list this week. Then build it into the beginning of each assessment cycle so it runs as prevention, not correction.
For context on how these same documentation gaps show up during survey, our SNF Survey Prep guide covers what surveyors look for in the same records from a different direction but with the same consequences. You may also find it useful alongside our breakdown of how payer mix affects your overall revenue picture and what the Illinois Medicaid rate environment looks like in 2026.
The Report Will Come Again Next Month
Imagine it arrives.
Finance opens the dashboard. The CMI number is there. And instead of the familiar dread the scramble to explain what happened, the conversation with the MDS coordinator that starts with “let’s look into it” you already know.
You knew three weeks ago. Because your workflow flagged two residents with incomplete Section GG before their ARDs closed. Because a new admission’s I0020B was corrected on day 2 after the hospital packet arrived. Because a resident who returned from the hospital on day 18 triggered a significant change conversation in morning meeting the same afternoon.
The report still arrives. But you are not reading it to find out what happened. You are reading it to confirm what you already fixed.
That is the difference between reacting to reimbursement problems and preventing them.
Every CMI drop starts as a workflow problem long before it becomes a finance problem. The facilities that understand that stop having the Monday morning conversation with finance because they had the Tuesday morning conversation with their MDS coordinator three weeks earlier.
That is also exactly why myMDS.ai exists. Not because it was a software idea someone had in a meeting because I ran St. Anthony’s Rehabilitation and Nursing Center in Rock Island, Illinois and kept having the reactive version of this conversation. We built myMDS.ai because the alternative was continuing to find out what went wrong after it was already too late to change it.
If that problem is familiar, let’s talk. Or take a broader look at what the LTC Apps platform covers across SNF operations.
The report will come again. The question is which version of that morning you are planning for.




